
This gallery contains 25 photos.
Browse the photo gallery below of the Naída CI Q70 and all its associated goodies. Click on an image to enter the slide show!

This gallery contains 25 photos.
Browse the photo gallery below of the Naída CI Q70 and all its associated goodies. Click on an image to enter the slide show!
From N5 to N6: Initial Impressions
A review of the Cochlear Nucleus 6

Model reviewed: CP910
To go from significant hearing loss to being able to hear significantly within the space of four weeks – the usual period between a cochlear implant operation and activation with the processor – is a life-changing experience for many. To then go from activation with one device to an upgrade to the latest processor for that device within three weeks was an equally life-changing moment for one London recipient.
TB is an adult cochlear implant user who received her first processor, a Cochlear Nucleus 5 (N5) in summer 2013. Three weeks after activation, she was upgraded to the Cochlear Nucleus 6 (N6) and the article below brings together her experiences since activation with those of a long-term user of the N5 who has not yet upgraded to the N6, to allow comparison of the models for the purposes of this review.
Both users are broadly similar in background and experience, being profoundly deaf from birth or infancy, and having grown up in mainstream education with good speech and lipreading skills. Both were motivated to obtain their cochlear implants through finding it increasingly difficult and demanding to keep up lipreading skills in their day-to-day lives. TB recalls “falling asleep through exhaustion” at the end of the day, while SC, a lifelong lipreader, found that she was forced to put in more and more effort to achieve the same results as she had had in her teens.
Distilling experiences between users of the N5 and the N6 with similar backgrounds provides a comparable benchmark between users, their expectations, and their experiences between two different models of the same brand of cochlear implant speech processor.
User experiences compared:
Both users found activation with the N5 an overwhelming experience, one that is common to many cochlear implant activations, regardless of brand or hearing history: it is in part attributable to the sudden access to a wider range of sounds than hitherto, rather than to the specific implant itself. Their reactions were surprisingly similar: “I hated it and thought to myself, what had I done?” (TB) and “So this is how hearing people hear, my goodness, I don’t know if I want to be part of this world!” (SC) Both adapted remarkably quickly to being able to hear again, and it appears that for TB access to the N6 has accelerated this process of adaptation.
TB exchanged her N5 for an N6 three weeks after activation, and reported an immediate positive response to the change in processor that seems to go beyond the changes expected at the key stage of mapping 1 month post-activation. (For comparison, at 1 month SC was given the basic map that she still uses for everyday purposes.) In particular TB reported that the automatic scanning of environmental sound as part of the N6’s new processing strategy (which is described in more detail below) significantly reduced the noise levels of a busy London street. Prior to this point she felt that she had been struggling with ‘loud noise syndrome’ in which she felt that her voice rose above the surrounding noise level, and the impact of the new strategy returned her voice to normal levels, much to her relief, as she was no longer straining to hear herself.
Description and technical features of N5 CP810 for comparison:
 The N5 CP810 sound processor has dual microphones alternating with dual control buttons across the top of the processor, with an accessory port hidden under a flap. The size of the processor can be modified to suit the user through battery choice, with three interchangeable battery options: a standard sized battery cage holding two cochlear-implant specific disposable batteries, and rechargeable lithium-ion batteries offered in two sizes: standard and compact.
The N5 CP810 sound processor has dual microphones alternating with dual control buttons across the top of the processor, with an accessory port hidden under a flap. The size of the processor can be modified to suit the user through battery choice, with three interchangeable battery options: a standard sized battery cage holding two cochlear-implant specific disposable batteries, and rechargeable lithium-ion batteries offered in two sizes: standard and compact.
 It is accompanied by the CR110 remote assistant in white with a large user-friendly central button, allowing the user to cycle between programmes remotely rather than through the buttons on the processor itself. SC found this useful in toggling between programmes in the early days of activation, rather than using the buttons on the processor. It also permits individual settings of volume and sensitivity across all four available programmes: Everyday, Noise, Focus, and Music, which in the CP810 can be loaded individually or collectively with the proprietary SmartSound strategy. Everyday and Music are self-explanatory; Noise is intended to reduce the discomfort of surrounding noise, while Focus is intended to enhance speech discernment in noise.
It is accompanied by the CR110 remote assistant in white with a large user-friendly central button, allowing the user to cycle between programmes remotely rather than through the buttons on the processor itself. SC found this useful in toggling between programmes in the early days of activation, rather than using the buttons on the processor. It also permits individual settings of volume and sensitivity across all four available programmes: Everyday, Noise, Focus, and Music, which in the CP810 can be loaded individually or collectively with the proprietary SmartSound strategy. Everyday and Music are self-explanatory; Noise is intended to reduce the discomfort of surrounding noise, while Focus is intended to enhance speech discernment in noise.
The remote assistant also allows a certain amount of troubleshooting via simple yes/no choice options to identify typical issues, reassuring for users (and which SC has only ever used twice in 3.5 years to solve simple issues).
Programming is flexible, with the capacity to have four programmes based on the same map or to tailor the programmes according to user preference. For example, the Noise and Focus programmes can be discarded if preferred and replaced with Everyday and Music programmes based on a second map, thus having a choice of two Everyday and two Music programmes for different listening situations.
Description and technical features of the new N6 CP910 and CP920 models:
Physical features:
 In appearance, the N6 is very similar to its predecessor, with some minor modifications that result in increased comfort. The controls and microphone covers are also similarly disposed alternately across the top of the processor, with greater ease of use in the control buttons. There are two models, the CP910 and CP920: the difference between the two models is that the CP910 offers an accessory hatch similar to the N5 for direct input of cables from audio accessories such as mp3 players, etc., while the CP920 does not, leading to a size reduction in the CP920.
In appearance, the N6 is very similar to its predecessor, with some minor modifications that result in increased comfort. The controls and microphone covers are also similarly disposed alternately across the top of the processor, with greater ease of use in the control buttons. There are two models, the CP910 and CP920: the difference between the two models is that the CP910 offers an accessory hatch similar to the N5 for direct input of cables from audio accessories such as mp3 players, etc., while the CP920 does not, leading to a size reduction in the CP920.
Like the previous generation N5 processor, the N6 CP910 and 920 are both powered by a rechargeable lithium-ion battery or disposable battery unit taking 2 cochlear implant-specific batteries. Both compact and standard size rechargeable batteries are available in the UK.[1] The compact batteries of the N6 and N5 differ very slightly in profile, the N6 having straight edges rather than being slightly rounded, shaving off a fraction of the size, up to 2mm in height.[2] However, the batteries of the two are interchangeable using the same snap-on/off mechanism, which is good news for those wanting to upgrade and having significant life remaining in their existing N5 batteries. It is also good news from an ecological standpoint.
The choice of a CP920 without an accessory hatch and powered by fractionally more compact batteries therefore reduces model size compared with the N5 CP810 in two dimensions, which is immediately apparent to the wearer. Most implant recipients will previously have worn hearing aids, which are nowadays extremely small: while cochlear implants do not currently match the small size of the latest hearing aids, the market as a whole is tending towards miniaturization of the external package. These changes, though cosmetic, represent a positive step forward in that direction for Cochlear and would be an attractive option for adults with small ears and for children. User comfort is an important consideration in encouraging implantees to wear their processors during waking hours to obtain maximum benefit.
The processing strategies have been refined with a wider suite of programmes for different hearing and listening situations to suit the user, although the processor still has a capacity of four programme slots.[3] The proprietary SmartSound iQ can be used as a programme in its own right, automatically scanning the ambient noise environment and responding with an appropriate selection out of six rather than four possibilities. This takes it beyond the previous generation SmartSound strategy on the N5, which could be layered across one or more programme slots to enhance that particular programme, but could not change the programme itself to suit the environment.
The original four programmes appear to have been retained as part of the choice for the user, two of which have been renamed to reflect the role they play more accurately: they are: Speech (Everyday); Noise; Speech in Noise (Focus); and Music. They are joined by Quiet, in which soft sounds are highlighted, and Wind, suppressing ambient wind noise, and the Smartsound iQ programme will select from all of these within its own programme slot. Each of these choices is available as a programme in its own right on the other slots.
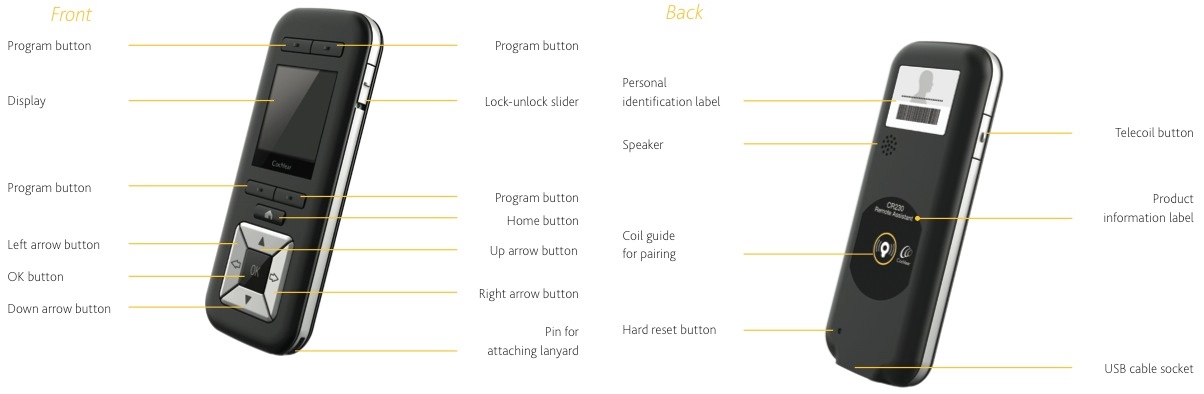 The CR230 remote assistant delivers the same programme selection and troubleshooting options as the former N5 model with a similar user-friendly large button, although it has been restyled and is much more mobile-phone like in appearance than the white N5 remote, and has a USB port for future data exchange capabilities.[4] The smaller CR210 remote control allows simpler adjustments to be made and could be useful for children or the elderly.
The CR230 remote assistant delivers the same programme selection and troubleshooting options as the former N5 model with a similar user-friendly large button, although it has been restyled and is much more mobile-phone like in appearance than the white N5 remote, and has a USB port for future data exchange capabilities.[4] The smaller CR210 remote control allows simpler adjustments to be made and could be useful for children or the elderly.
Data Logging:
In tandem with the upgrade to automatic scanning, the N6 processor also differs from the N5 in that it also offers a data logging capability.[5] This can: show how long the processor is in use on a daily basis; identify to the audiologist which programmes the user prefers; and demonstrate noise levels of exposure, permitting the programmes to be tailored more specifically to user needs, again a refinement which reflects a wider trend in the cochlear implant world.[6] These are lifestyle options and it is easy to envisage that someone who lives an outdoor lifestyle will, for example, appreciate the benefits of enhancing their maps to minimise wind noise.
For example, the Quiet programme was a good choice for TB in her earlier maps as she adjusted to learning to hear again, but this has now been discarded in favour of enhanced remaps on the ‘scan’, speech and music slots, with the standard industry ‘good practice’ of saving a previous favourite, in this case an earlier map on her previous ‘scan’ programme, as a fall-back. The ‘scan’ programme is currently the programme which TB uses 90% of the time and she reports that her most recent map has “given me a boost to the noise levels, rather than set the electrodes individually.”
The ability to respond to the ambient sound environment in several different ways has enhanced the ‘new user’ experience for TB, who has only been activated for a few months. Her sound environment has altered radically from that initially rather unpromising start, so much so that she “finds the sound of light wind really rather relaxing.” That, in the end, is what it is all about: discovering the world of sound, all the myriad little things that hearing people ignore or take for granted.
*One final aspect of the N6 cannot yet be reviewed – the advertised wireless capability which remains in development and is not yet available. It is understood that it will become available to current and new users via a software upgrade. Hence the title of this review: From N5 to N6, Initial Impressions to allow for a follow-up review.
With many thanks to TB for her willingness to share her new user experiences and compare and contrast the N5 with the N6, and to Howard Samuels for his support and suggestions.
Tamara Bunting is a researcher with a leading medical charity in London, UK.
 Serena Cant is a researcher in one of the main UK heritage organisations, and blogs regularly on her experiences of her cochlear implant, together with arts reviews and musings on being deaf, at deaflinguist.wordpress.com.
Serena Cant is a researcher in one of the main UK heritage organisations, and blogs regularly on her experiences of her cochlear implant, together with arts reviews and musings on being deaf, at deaflinguist.wordpress.com.
[1] Not yet approved by the FDA in the US at the time of writing. Cochlear: Options to suit your lifestyle
[2] Measurements in two dimensions taken and cross-checked by TB and SC, October 2013.
[3] Cochlear: SmartSound iQ and as reported by TB, October 2013.
[5] Cochlear: Nucleus 6 Canadian Announcement with mention of datalogging capability and audiological session, TB, October 2013
[6] Personalizing maps even for long-term implant patients, has been a focus of recent research: for example, the recent Vanderbilt study.
Welcome to our new feature – CochlearimplantHELP Comics! If you’d like to submit comics or even suggestions, feel free to contact us!

(click on comic to enlarge)
Thanks to Stephan Pretorius for today’s submission!
Two Scientists Who Received the Prestigious Lasker Award and Major General USMC to Speak on Cochlear Implants
WHAT: The Cochlear Implant 2013 Symposium, a national conference of cochlear implant clinicians, will honor two scientists, Dr. Ingeborg Hochmair and Dr. Blake Wilson, who recently received the prestigious Lasker Award for Clinical Medical Research, often referred to as the “American Nobel Prize.” These scientists developed and improved the cochlear implant, allowing deaf patients to hear, transforming lives and for the first time, restoring a human sense with a medical intervention through their pioneering work.
Major General Robert Hedelund, USMC, will also be on hand to discuss cochlear implantation as a solution for the number one health issue facing combat duty personnel—substantial hearing loss incurred during their service to our country.
A highlight of the symposium is the premiere of the new dramatic film, 95 Decibels, followed by a panel discussion with the director, crew and actors, Oct. 24 from 6:30 to 7:45 p.m. The movie chronicles the true story of a family whose daughter was diagnosed as profoundly deaf at 18 months of age and the obstacles they faced.
WHO: American Cochlear Implant Alliance is a non-profit dedicated to improving access to cochlear implantation through research, advocacy and awareness.
Available for interviews:
WHY: Expand awareness of the power of cochlear implants today. Only 6% of eligible individuals in the US currently have a cochlear implant. Deafness can be helped.
WHEN: Thursday, October 24, 1:00 PM
WHERE: Hyatt Regency Capitol Hill, 400 NJ Avenue NW, Washington, DC. Street parking and hotel valet.
RSVP: More information and to schedule an interview: www.acialliance.org and Donna Sorkin, dsorkin@aciallance.org (cell) 703.585.7336
Charlie Rose dedicated an episode of his television show to examine cochlear implants, and to help understand the impact the recipients of the 2013 Lasker-DeBakey award have had.

Blake WIlson
Three giants in the field of cochlear implant research have received the prestigious 2013 Lasker~DeBakey Clinical Medical Research award for the development of the modern cochlear implant.
Graeme Clark, whose efforts led to the commercially available implants at Cochlear Ltd, and Ingeborg Hochmair, whose parallel efforts led to the MED-EL Corporation’s cochlear implants, have relentlessly pursued the monumental engineering and biological challenges of creating the most successful neural prosthesis by far.
While the original multi-channel cochlear implants afforded most recipients access to sound, many still needed to rely on contextual or visual cues to understand speech. These early implants were marvels of engineering, science, and biotechnology. However, without advanced stimulation protocols, they were like powerful computers without software that fully exploited their capabilities.
Blake Wilson and colleagues developed a new stimulation protocol comprising a number of key elements. This method, known as CIS (Continuous Interleaved Sampling) provided an immediate and dramatic improvement in cochlear implant performance, and is the basis for stimulation in all modern cochlear implants.
Early in the process of exploring different protocols (funded primarily by the National Institutes of Health), Blake Wilson’s team at Research Triangle Institute in North Carolina recommended that the results from the research be donated to the public domain, forgoing potentially enormous personal and organizational royalties and other income. This supremely altruistic choice enabled as many people as possible to achieve maximum benefit from cochlear implants. Given that the cumulative global sales of cochlear implants is on the order of ten billion dollars, Wilson’s own estimate of the cost of that decision in the tens of millions appears to be quite conservative.
Indeed, without this one selfless act, cochlear implants would not have become nearly as effective or widespread, and outcomes would not even come close to what we can expect from a modern cochlear implant.
Without volunteer test subjects, none of the research would have been possible. Many cochlear implant users have donated countless hours to research. These efforts continue today, and are always rewarded with gratitude from the researchers.
To explore different stimulation protocols, the researcher would prefer to have direct access to the individual electrodes. Today’s cochlear implants are quite sophisticated, and interpose a significant amount of electronics between the external interface and the actual electrodes.
Much of the testing during the development of CIS was conducted with subjects implanted with the Ineraid device. This implant had a percutaneous connector, ideal for applying experimental stimulation strategies. The Ineraid device is no longer manufactured.
Compressed Analog, one of the more straightforward early strategies available prior to CIS, compresses the wide dynamic range of sound into the more limited electrical dynamic range needed for electrical stimulation. The signal is then split it into frequency bands to be presented to the individual electrodes.
This method mimics the natural hearing process, although the number of electrodes is minuscule compared to the number of hair cells in the cochlea. The thought behind the CA strategy is to present the brain with as much information as possible, and to rely on the brain to process this rich information set.
Because all electrodes are stimulated continuously and simultaneously, uncontrolled interactions between channels degrade performance.
In order to reduce interaction between channels, the electrodes may be stimulated at different times. Each electrode presents a pulse proportional to the signal strength in that channel. Because only one electrode is stimulated at any given time, channel interactions are greatly decreased.
Applying this Interleaved Protocol at a much higher rate for the whole array of electrodes is a key feature of CIS.
Other early strategies included feature extraction, which attempted to present primarily the important parts of sound for speech comprehension. Eventually it was determined that presenting as much information as possible, and letting the brain sort out the speech, proved to engender the best performance of the different approaches.
CIS is a combination of new and existing elements, which when used together, dramatically improve the performance of subjects using cochlear implants. Rather than a pre-packaged library of software, CIS is implemented in a custom manner for each cochlear implant system. All modern protocols are based on CIS, with various enhancements and refinements. The elements of CIS include:
According to the Lasker~DeBakey Clinical Medical Research Award Description, ‘…Wilson’s “continuous interleaved sampling” (CIS) system has allowed the majority of cochlear implant recipients—for the first time—to understand words and sentences with no visual cues. CIS supplies the basis for the sound-processing strategies that are now widespread and fueled an exponential growth in implant use that began in the early 1990s. Its rapid introduction, utilization, and dissemination stemmed in large part from a policy that donates to the public domain all intellectual property produced by Wilson and his colleagues from their NIH-funded cochlear-implant research.’
The global cochlear implant community, and indeed society as a whole, owe Blake Wilson a tremendous debt of gratitude for his seminal contributions to the field.
Symbion, the company that made Jarvik 7 artificial hearts, also made a brief foray into cochlear implants. The company was subsequently purchased by Richards Medical Company, a member of the Smith+Nephew group. The processors may be branded either Symbion or Smith+Nephew. The Ineraid implant is quite simple – several electrodes attach to a percutaneous connector – one that goes through the skin.
The implant received an FDA investigational device designation, and a hundred or so patients were implanted beginning in 1985. The volunteers who considered participating in the clinical trial received this information guide. The device never received FDA approval, as transcutaneous devices with magnetic headpieces became the preferred choice in the marketplace.
The Owner’s Handbook includes tips for self-guided rehabilitation therapy, how to carry a spare battery, and how to care for the pedestal to prevent infections.
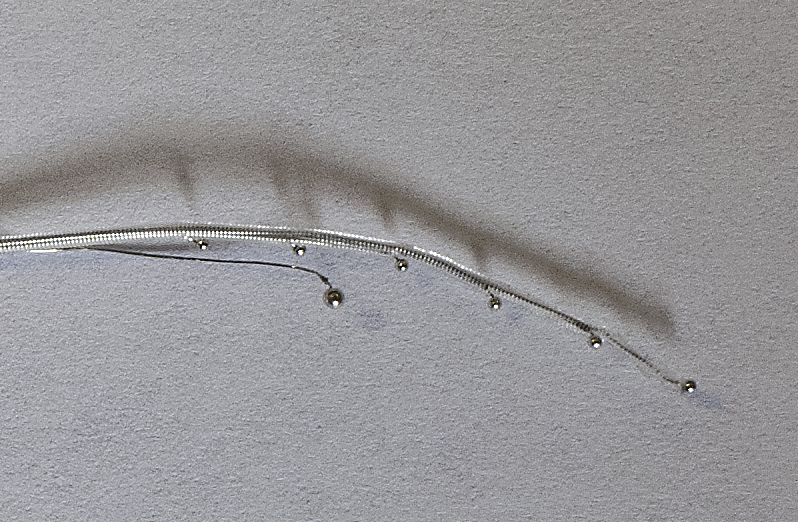
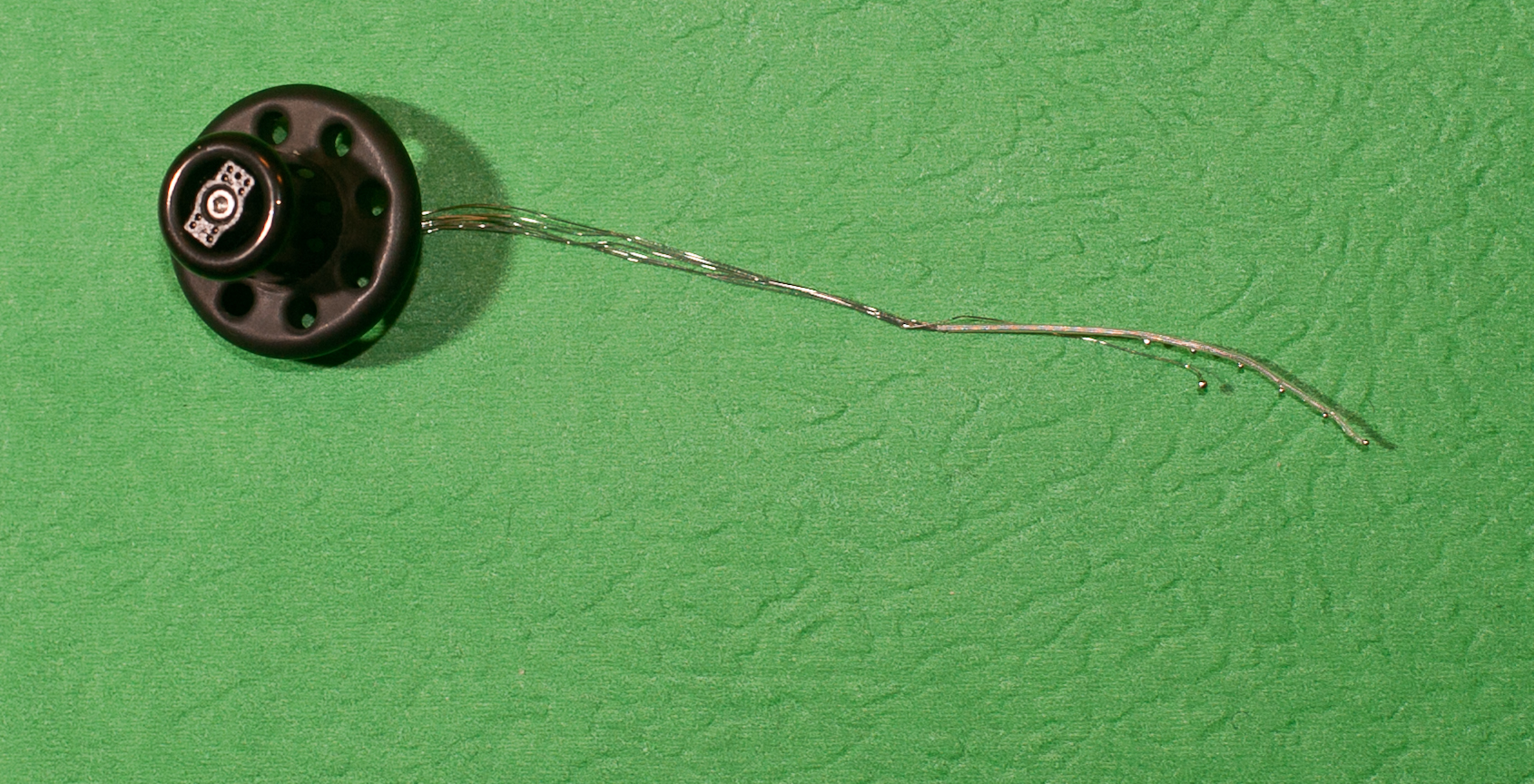
The six balls along the main part of the array are the active electrodes. The ground, or reference electrode, is the larger ball on a separate wire. The outer ring of the black pedestal is affixed to the skull, and the inner portion comes through the skin where the external processor makes its connections to the electrodes.

The processor is housed in an aluminum case, and has only two controls – power/volume, and sensitivity. A panel slides off to reveal a compartment for a standard 9V battery.


The ear hook assembly connects to the body-worn processor with a cable. The cable has one wire for each electrode, plus the ground wire. The black wire coming out of the earhook goes to a connector that plugs onto the pedestal. This performs the same function as the headpiece in modern cochlear implant systems.

This simple arrangement was specifically chosen to be upgradeable using only external components. Any advances in electronic hardware and software can be implemented with external components alone, requiring no further surgery.
The microphone port is visible in this view of the ear hook. It appears to be a precursor to today’s T-mic from Advanced Bionics.

Direct access to the electrodes of the Ineraid device makes it an ideal vehicle for testing new stimulation strategies. The original processor does not have the desired flexibility for research purposes. While the electrodes can be stimulated in the laboratory environment, a wearable processor would enable volunteers to try different strategies for longer periods of time.
To that end, researchers at the Massachusetts Eye and Ear Infirmary Cochlear Implant Research Lab and at the University of Geneva arranged for the production of the Geneva processor. The National Institutes of Health (NIH) funded the project in the United States. Hardware design and fabrication were done by engineers at the Geneva School of Engineering.
The purpose of the Geneva processor was to provide a wearable platform on which new speech processing strategies could be evaluated with long term use, as opposed to testing during brief visits to the research labs. One of the first and most important strategies tested was the CIS strategy, which had already demonstrated superior results in the lab.
There were about 20 Geneva subjects in the US and a similar number in Europe. About half of them are still using the devices on each continent.

The MED-EL CIS LINK
In 1995, MED-EL developed the CIS LINK, an ear hook to interface between the MED-EL processor of the time, and the Ineraid implant. Because the processors expected to interface to the internal electronics of the MED-EL implant, this earhook incorporated the electronics of the MED-EL implant, providing the critical piece of interface electronics.

This system gave Ineraid users access to CIS. Their involvement as test subjects proved instrumental in the development of the algorithm. MED-EL says:
‘Out of humanitarian reasons an addition to the CIS PRO+, the CIS LINK system, is developed to provide the CIS strategy to Ineraid recipients who had received percutaneous plug CI systems by another company which discontinued further development.’
 We’ve all heard about Jacob getting clipped by a truck (hit and run), just 180 miles short of his final stop in the 11,000 mile tour to raise funds for cochlear implant charities. From Jacob’s Ride:
We’ve all heard about Jacob getting clipped by a truck (hit and run), just 180 miles short of his final stop in the 11,000 mile tour to raise funds for cochlear implant charities. From Jacob’s Ride:
Here’s what you can do:
 Jacob Landis has been bicycling all spring and summer to every MLB ballpark to raise money for cochlear implant charities. After nearly 11,000 miles, a chase van that died, and 180 miles short of his final stop, he posts:
Jacob Landis has been bicycling all spring and summer to every MLB ballpark to raise money for cochlear implant charities. After nearly 11,000 miles, a chase van that died, and 180 miles short of his final stop, he posts:
“Got hit by a tractor trailor’s mirror tonight less than 4 miles to the end of the ride. Concussion and a pretty bad left arm. I am only 180 miles from the last stop in Miami but cant finish the ride because of the arm. Spent a while in the ER.”
Link to this page on FB, share it, spread the word. Contribute if you haven’t already, or again if you have! Let’s all help him ride a wave of support into Miami!

Graeme Clark joins Ingeborg Hochmair and Blake Wilson in receiving the 2013 Laser~DeBakey Clinical Medical Research Award for the development of the modern cochlear implant. Read Cochelar’s press release here.
